ウェルナー症候群

千葉大学大学院医学研究院
内分泌代謝・血液・老年内科学
千葉大学病院
糖尿病・代謝・内分泌内科 / 血液内科 / 高齢者医療センター
ウェルナー症候群に対するニコチンアミド リボシドの安全性・有効性を検証するための前向き、単施設試験 ( EMPOWER試験 )
ウェルナー症候群には根本的治療法がなく、難治性潰瘍やサルコペニア、動脈硬化性疾患などへの対処療法が中⼼ですが、効果は限定的であり、更なる有効性が期待される治療法が必要とされています。
近年、老化に対する研究でサーチュイン遺伝子が見いだされました。サーチュイン遺伝子とは長寿遺伝子とも抗老化遺伝子とも呼ばれ、活性化される事により寿命が延びるとされています。このサーチュインの活性化にはNAD(ニコチンアミドアデニンジヌクレオチド)が重要とされています。ウェルナー症候群患者さんでは、このNAD値の低下を認めており(Nat Commun. 2019 Nov 21;10(1):5284.)、NADの元となる物質 (前駆体) の補充が有効である可能性があります。
千葉大学では、難治性潰瘍やサルコペニア、動脈硬化性疾患などの⽼化の抑制に効果的であるとされるNADの前駆体である「ニコチンアミド リボシド」のウェルナー症候群の患者さんに対する安全性及び有効性を検討するEMPOWER試験を実施しており、2021年9月末まで症例の募集を行っています。
試験の詳細をご覧になりたい方は、こちらをご覧下さい。
https://jrct.niph.go.jp/latest-detail/jRCTs031190141
ウェルナー(Werner)症候群は、1904年にドイツの医師オットー・ウェルナー(Otto Werner)により初めて報告された稀な遺伝病です。この病気は、思春期を過ぎる頃より急速に老化が進んでいくようにみえることから、「早く老いる」病気=早老症のひとつといわれています。20歳代から白髪、脱毛、両目の白内障がおき、手足の筋肉や皮膚もやせて固くなり、実年齢より「老けて見える」ことが多くなります。糖尿病や脂質異常症(コレステロールや中性脂肪の異常)も多く、かつては多くの患者さんが40歳代で悪性腫瘍や心筋梗塞などにより亡くなっていました。今では治療法の進歩により寿命が延びて50~60歳代の方もいらっしゃいます。その一方で足先や肘などの深いキズがいつまでも治らず(難治性皮膚潰瘍)、感染を繰り返して足を切断してしまうなど、なお多くの患者さんが大変な日常生活の苦労を強いられています。
いくつかの研究により、日本のウェルナー症候群の患者数は約2,000名、病気になる確率はおよそ5~6万人に一人と推定されています。
地域的には、世界中で報告されている患者さんのうち約6割が日本人であり、我が国に多いと考えられています。また以前は、主に血縁が濃くなる近親婚(いとこ婚やはとこ婚)の多い地域で報告されてきましたが、最近では近親婚によらない発病者も増加しています。日頃の食べ物や運動などの生活習慣は、発病とは関係ないと考えられています。
WRNと呼ばれる遺伝子の異常が原因と考えられています。私たちのからだの設計図であるDNA※1が傷ついた時に修理する役割を担っているのがWRN(DNAヘリカーゼともいう)です。しかし、WRNの異常によりなぜ老化が早く進むようになるのかはまだ分かっていません。
ヒトは両親からもらった遺伝子を一対(2つ)ずつ持っています。ウェルナー症候群は2つのWRN遺伝子の両方に異常がある時だけ発病します。患者さんの両親はそれぞれひとつだけ原因遺伝子を持ち、ご自身は発病していないケースがほとんどです。患者さんの兄弟姉妹では確率的に約4人に1人が発病しますが、患者さんのお子さんや、さらにそのお子さんが同じように発病する確率は計算上200~400人に1人以下であり、結論として可能性は非常に少ないです。
20歳代以降に白髪・脱毛などの毛髪の変化や、白内障(両目の場合が多い)、かん高くかすれた声などの症状がおきてきます。また腕や脚の筋肉がやせ、皮膚も固く薄くなり、深いキズができて治りにくくなります(難治性皮膚潰瘍)。身長は低いことが多く、レントゲンではしばしばアキレス腱や皮下の石灰化(カルシウム成分が溜まること)が見つかります。また糖尿病や脂質異常症になる方が多く、性ホルモンの働きが落ちてくる更年期なども早い年齢から起こりやすくなります。
ウェルナー症候群にはまだ根本的に治す方法がなく、白髪や脱毛、皮膚の変化など「見た目の老化」にも治療や予防方法がありません。足のキズは治りにくく、日常生活に大きな支障をきたしますので、靴ずれを起こさない、などの予防が重要です。できてしまった場合には、洗浄や消毒・保護・保湿などの対症療法が中心になりますが、自分のからだの他の場所から皮膚を移植する手術が有効な場合もあります。一方、悪性腫瘍や白内障、糖尿病や脂質異常症などは、一般患者さんと同じ様に手術や投薬などが有効であり、早期発見と治療が重要です。
かつては、悪性腫瘍(がん)もしくは心筋梗塞など動脈硬化の病気によって、多くの患者さんが40歳代半ばで亡くなると言われていました。しかし、最近の研究によると平均寿命が10年以上延び、今では60歳代の患者さんも増えています。一方で、患者さんの多くがかかとや足、肘などに治りにくいキズ(難治性皮膚潰瘍)を患い、痛みや感染が続いて足を切断せざるを得ない状況にも至るなど、日常生活に支障を来すようになっていくことが大きな問題です。
まず、治りにくい深いキズ(難治性皮膚潰瘍)ができないように、日頃からアキレス腱やかかと、足、肘など潰瘍になりやすい部位をなるべく保護し観察することです。薄く固くなった皮膚は骨に圧迫されてキズができ、やがて深い潰瘍を生じやすいため、当たって痛い箇所やキズになりかけたところは特殊な靴(装具)を作って保護する方法もあります。また定期通院により悪性腫瘍の発症をチェックしたり、糖尿病や脂質異常症などの代謝異常を治療・管理して動脈硬化が早く進むのを防いだりすることも大切です。
※1 DNA:
人体を構成する細胞の中にある物質で、生命を維持するために必要なタンパク質をつくる設計図の役割をもつ
※ウェルナー症候群ハンドブック
ウェルナー症候群の皆さんと家族・医療者のためのガイド 第1版

確定: 主要徴候の全て。もしくは3つ以上の主要徴候に加え、遺伝子変異を認めるもの
疑い: 主要徴候の1、2に加えて主要徴候やその他の徴候から2つ以上。
「ウェルナー症候群の診断・診療ガイドライン」26ページ掲載Takemoto M,Mori S,Kuzuya M,Yoshimoto S,Shimamoto A,Igarashi M,Tanaka Y,Miki T,and Yokote K,Diagnostic criteria for Werner syndrome based on Japanese nationwide epidemiological survey. Geriatr Gerontol Int. 2012, in press
http://www.nanbyou.or.jp/entry/5321

若年ウェルナー症候群の遺伝子診断
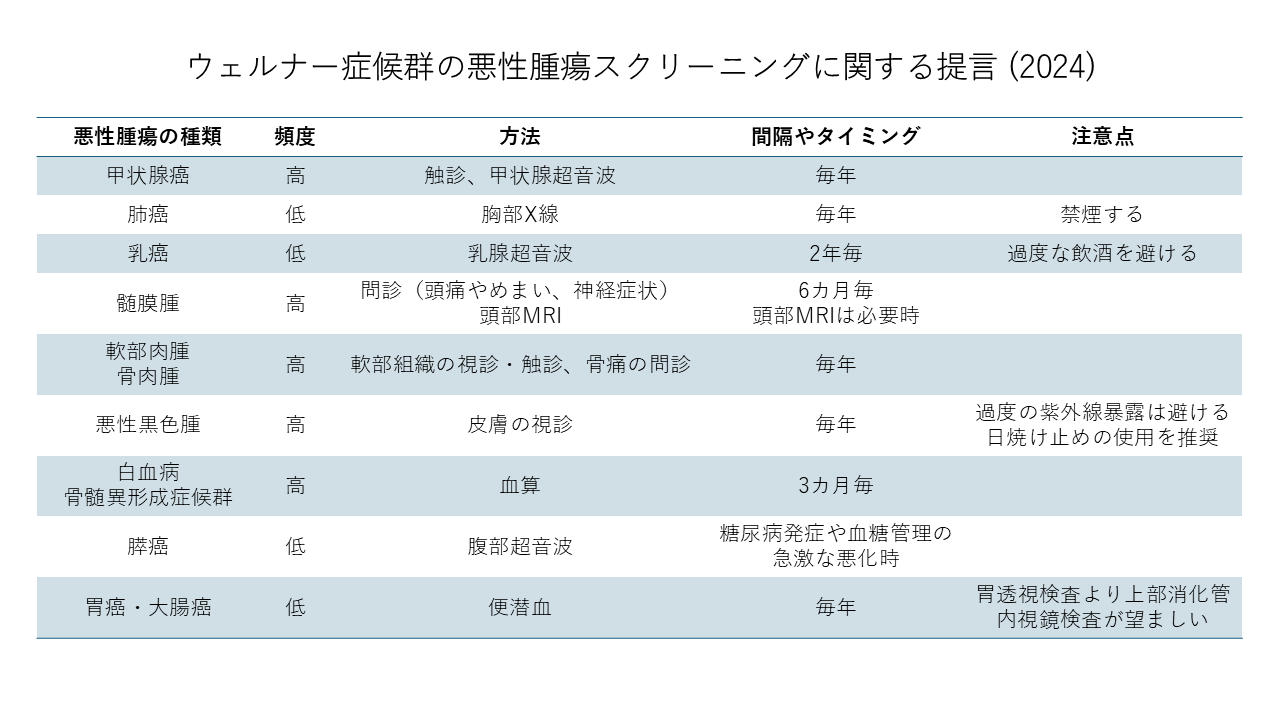
ウェルナー症候群がんスクリーニング
本ホームページでの無修正での画像・音声を呈示することに対し、積極的なご賛同のご承諾を頂いています。
画像・音声の無断転用を堅くお断りします。
このたび、日本医療研究開発機構(難治性疾患実用化研究事業)「早老症ウェルナー症候群の全国調査と症例登録システム構築によるエビデンスの創生」により、本邦におけるウェルナー症候群の実態を把握するために全国疫学調査を実施しております。
ウェルナー(Werner)症候群は、稀な遺伝的早老症であり、世界中で報告された症例の3分の2が日本人というわが国に頻度が高い疾患です。2009年にも全国調査を行ない、皆様に御協力頂きました。その結果、約200名ウェルナー症候群患者が見出され、同疾患が難病指定を受ける契機となりました。またこの調査結果をもとにウェルナー症候群の診断基準が25年ぶりに改訂され、これまでなかった治療ガイドラインが作成されました。現在国内には約2000人の患者数が推定されていますが、その現状は十分に把握されておらず、未だ根治療法もありません。そこで、患者の生命予後やQOLを改善するために有用な日本発のエビデンスの構築を目指しています。
今回の調査においても、約半数の御施設から御回答頂いており、大変感謝申し上げます。アンケート調査を送らせて頂いた御施設で、御返信頂いていない御施設の御担当の先生で御回答頂けましたら、御多忙のところ誠に恐縮ですが、過去10年の貴診療科における該当患者様もしくは該当疑い患者様の患者数を同封の調査用紙に御記入の上、FAX(043-226-2095)にて御返信下さい。該当する患者様が不在の場合にも、全国の患者数推計に必要ですので、調査用紙の「なし」にマークをつけ、御返送下さいますようお願い申し上げます。
また、新たな患者様を診察された先生からの御連絡や遺伝子検査の御依頼も受け付けております。
お送りしましたアンケート調査票と添付の資料は、こちらからもダウンロードいただけます。
該当するもしくは該当することが疑わしい患者様ありの場合には、後日調査個人票を送 付させて頂く可能性があります。その場合にはあわせて御協力下さいますよう重ねてお願い申し上げます。
本調査によってウェルナー症候群の症例登録システム構築を推進し、治療ガイドラインの改訂を通じて、同疾患の診療の質を向上し、患者様の予後改善に貢献できるよう班員一同努力して参る所存です。何卒ご協力を賜わりますよう、よろしくお願い申し上げます。
ウェルナー症候群 全国疫学調査事務局: 〒260-8670 千葉市中央区亥鼻 1-8-1
千葉大学大学院医学研究院 内分泌代謝・血液・老年内科学
日本医療研究開発機構 難治性疾患実用化研究事業
「早老症ウェルナー症候群の全国調査と症例登録システム構築によるエビデンスの創生」
研究班
研究代表者 横手 幸太郎
ウェルナー症候群 全国疫学調査担当 越坂 理也
(千葉大学大学院医学研究院 内分泌代謝・血液・老年内科学)
電話:043-226-2092、 FAX:043-226-2095
日本医療研究開発機構(難治性疾患実用化研究事業)「早老症ウェルナー症候群の全国調査と症例登録システム構築によるエビデンスの創生」により我が国におけるウェルナー症候群の実態を把握するための平成29年度全国疫学調査(一次調査)を行いました。その結果がまとまりましたので、公表いたします。
本調査は、平成29年2月から全国の200床以上の病院の7889の診療科(内科、眼科、皮膚科、整形外科、形成外科など)を対象としてアンケートの形式で実施しました。計3154通(回収率40%)と多数の御回答を頂くことができ、御協力頂きました各施設の先生方に、この場をお借りして改めて御礼を申し上げます。
平成22年に実施した前回の全国調査の結果、約200名ウェルナー症候群患者さんを見出すことができましたが、今回の調査では、新たに男性57名、女性59名、計116名のウェルナー症候群患者さん(確定症例)の存在が明らかになりました。このほか、ウェルナー症候群が疑われる患者さん(疑い症例)も、男性29名、女性22名、計51名いらっしゃることが分かりました。ウェルナー症候群が疑われる患者さんに関しましては、現在、当教室で遺伝子検査を実施中です。さらに、過去10年間に、全国いずれかの医療機関へ通院されたことのある診断が確定した患者さん(過去通院確定症例)も、男性80名、女性71名、性別不明2名と計153名を把握することができました。すなわち、日本国内に、確定症例、疑い症例、過去通院症例の総計320名の患者さんの存在が明らかになりました。
| Werner 確定 症例 男性 | Werner 確定 症例 女性 | Werner 疑い 症例 男性 | Werner 疑い 症例 女性 | Werner 過去通院 確定症例 男性 | Werner 過去通院 確定症例 女性 | 総計 | |
|---|---|---|---|---|---|---|---|
| 小計 | 57 | 59 | 29 | 22 | 80 | 71 | |
| その他 | 性・数不明2 | ||||||
| 合計 | 116 | 51 | 153 | 320 | |||
また、全国における患者さんの分布については、地域的な偏り*が見られませんでした。したがって、その発症頻度に明らかな地域差はなく、日本国内に広く患者さんが存在することが示唆されます。
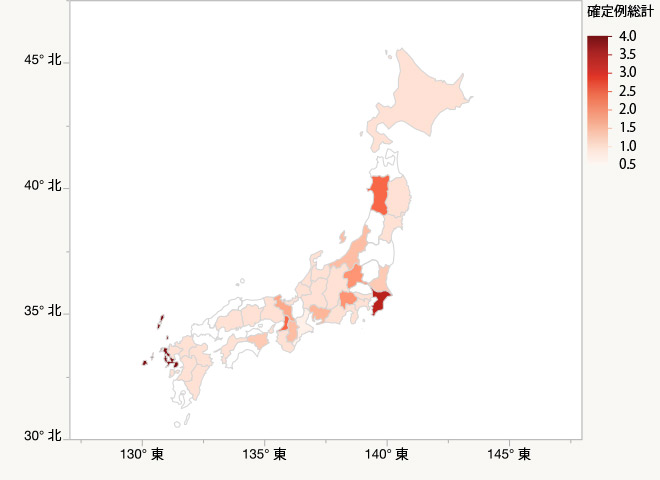
確定症例
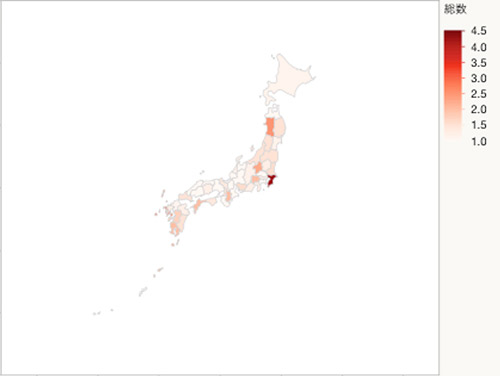
確定症例+疑い症例+過去通院確定症例
一次調査で確定診断例を御報告下さった御施設を対象に、今後二次調査を実施させて頂く予定です。二次調査ではウェルナー症候群の症例登録(レジストリ)システムを用いて、得られた情報をもとに、疾患の調査、治験**などの研究への募集、登録患者さんおよび主治医の方への情報提供などに活用して参る所存です。
今回の一次調査は終了しましたが、新たに患者さんを診察された医師の皆さんからの御連絡や遺伝子検査の御依頼も随時受け付けております。
* 他県に比べ、千葉県での報告が多くなっていますが、これは千葉大学病院に多くの患者さんを御紹介頂いているためと考えられます。
**大阪大学の中神医師を中心として、本年9月から行われる「新規ペプチドを用いた難治性潰瘍」の治験への参加を希望される患者さんを募集しています。このほか、千葉大学では、iPS細胞を用いた研究も行っています。
ウェルナー症候群 全国疫学調査事務局: 〒260-8670 千葉市中央区亥鼻 1-8-1
千葉大学大学院医学研究院 内分泌代謝・血液・老年内科学
日本医療研究開発機構 難治性疾患実用化研究事業
「早老症ウェルナー症候群の全国調査と症例登録システム構築によるエビデンスの創生」
研究班
研究代表者 横手 幸太郎
ウェルナー症候群 全国疫学調査担当 越坂 理也
(千葉大学大学院医学研究院 内分泌代謝・血液・老年内科学)
電話:043-226-2092、 FAX:043-226-2095

国際シンポジウム・早老症と関連疾患2018
International Meeting on RECQ Helicases and Related Diseases 2018
会期:2018年2月16日(金)-18日(日)
会場:かずさアカデミアパーク
URL:http://www.jtbw-mice.com/recq2018/
本会は爾来、ウェルナー症候群、ブルーム症候群、ロスムンド・トムソン症候群のRECQヘリカーゼ関連早老症候群を対象として米国で行なわれてきました。今回はアジアで初めての開催にあたり、色素性乾皮症、コケイン症候群、そしてハッチンソン・ギルフォードプロジェリア症候群を加え、さらに関連する細胞老化、ミトコンドリア障害、iPSバイオロジーなど幅広い老化関連研究を包含しての開催となりました。総勢135名(うち29名が外国人)の参加を得て、非常に盛会となりました。12人の外国人を含む27人の演者からご講演を頂き、いずれもハイレベルな内容で、ディスカッションも大いに盛り上がりました。海外からの5名を含む計21名の患者様、ご家族も参加され、研究者と患者の間に活発な交流が生まれています。国内外の参加者から、患者さんとの交流により課題がはっきりし、よりモチベートされたという声をいただくなど、ユニークなシンポジウムとなりました。

2016年5月28日~30日に米国ワシントン州シアトル市で早老症に関する国際シンポジウムRECQ2016が開催されました。
RECQ型DNAヘリケースの遺伝子変異によって生じるウェルナー症候群やロスムンド・トムソン症候群、ブルーム症候群の診療と研究を行なう医師・研究者が最先端の研究発表を行なったほか、これら疾患の患者や家族が世界中から一同に会し、互いの交流を深めました。
千葉大学からは横手教授が招待講演を行なったほか、清水孝彦准教授、澁谷修一研究院が研究成果を一般演題として発表し、活発な討議が行われました。
会期中に開催された組織委員会において、次回2018年の同シンポジウムを日本で開催することが要請されました。

平成27年10月19日~22日にタイのチェンマイで開催された第10回国際老年学会議において研究代表者 横手幸太郎教授がsubmitted symposiumを組み、横手先生ならびに分担研究者の森聖二郎先生、葛谷雅文先生、竹本稔先生が発表を行い、研究成果の国外への発信、早老症に関する啓蒙、国外の老化研究者とのディスカッションを行いました。
米国University of Washington(シアトル)における講演で、研究代表者 横手幸太郎教授が早老症研究の成果を紹介し、今後の共同研究につながる討議を行ないました。
令和6年度 第1回班会議
2024年9月18日(水)
Web会議
2024年3月14日(木)
Web会議
2023年10月10日(火)
Web会議
2022年8月17日(水)
Web会議
2021年8月13日(金)
Web会議
2020年10月2日(金)9:00~10:00
Web会議
2020年3月27日(金)15:00~16:00
Web会議
2019年9月13日(金)
フクラシア丸の内オアゾD会議室 14:00~15:00
2018年8月16日(木)
フクラシア東京ステーション 6G会議室 15:00~16:30
2018年2月16日(金)
かずさアカデミアホール 会議室202A 17:00~18:30
2017年9月8日(金)
フクラシア東京ステーション 12:30~14:30
2017年3月26日(日)
AP東京八重洲通り 11F 会議室O 14:00~15:00
2016年8月18日(木)
フクラシア東京ステーション 6F 会議室D 15:00~16:00
2016年2月28日(日)
フクラシア東京ステーション 5F 会議室I 13:00~14:00
2015年8月13日(木)
TKP東京駅前カンファレンス ミーティングルーム9B 17:00~18:00
2015年2月27日(金)
TKP東京駅前カンファレンス ミーティングルーム5B 13:00~14:00
2014年6月23日(月)
アットビジネスセンター東京駅 303号室 18:00~19:00
2020年10月2日(金)10:00~11:00
Web会議
2020年3月27日(金)15:00~16:00
Web会議
2019年9月13日(金)
フクラシア丸の内オアゾD会議室 14:00~15:00
2018年8月16日(木)
フクラシア東京ステーション 6G会議室 15:00~16:30
2018年2月16日(金)
かずさアカデミアホール 会議室202A 17:00~18:30
2017年9月8日(金)
フクラシア東京ステーション 12:30~14:30
2017年3月26日(日)
AP東京八重洲通り 11F 会議室O 15:00~16:00
2016年8月18日(木)
フクラシア東京ステーション 6F 会議室D 16:00~17:00
2016年2月28日(日)
フクラシア東京ステーション 5F 会議室I 14:00~15:00
2015年8月13日(木)
TKP東京駅前カンファレンス ミーティングルーム9B 18:00~19:00
2015年2月27日(金)
TKP東京駅前カンファレンス ミーティングルーム5B 14:00~15:00
2014年6月23日(月)
アットビジネスセンター東京駅 303号室 19:00~20:00
2013年6月4日~6日
大阪国際会議場
招聘講演
「The Roles of Nature, Nurture and Chance in the Genesis of Variable Trajectories of Aging」
George M. Martin, M.D.
(Professor of Pathology Emeritus University of Washington)
「ヒトから学ぶ老化機構」
大島 淳子
(Research Associate Professor, Department of Pathology University of Washington School of Medicine)

2012年2月19日 13時00分~17時30分
東京国際フォーラム
2011年10月17日 18時30分~20時30分
東京ステーションコンファレンス
2011年2月2日 18時30分~20時30分
東京ステーションコンファレンス
2010年7月9日 18時30分~20時30分
コンファレンススクエア エアプラス ルームA
2010年2月17日 18時30分~20時30分
コンファレンススクエア エアプラス ルームA
2009年8月7日
カンファレンススクエア エムプラス ルームA
The clinical characteristics of Asian patients with classical-type Hutchinson-Gilford progeria syndrome.Sato-Kawano N, Takemoto M, Okabe E, Yokote K, Matsuo M, Kosaki R, Ihara K. J Hum Genet. 2017 Dec;62(12):1031-1035. doi: 10.1038/jhg.2017.90. Epub 2017 Sep 7.
Maezawa Y, Kato H, Takemoto M, Watanabe A, Koshizaka M, Ishikawa T, Sargolzaeiaval F, Kuzuya M, Wakabayashi H, Kusaka T, Yokote K, Oshima J.(2018) Biallelic WRN mutations in newly identified Japanese Werner Syndrome patients. Mol Syndromol. 2018 Jul;9(4):214-218.
Oshima J, Kato H, Maezawa Y, Yokote K.(2018)RECQ helicase disease and related progeroid syndromes: RECQ2018 meeting. Mech Ageing Dev. 2018 Jul;173:80-83.
Nakagami H, Sugimoto K, Ishikawa T, Fujimoto T, Yamaoka T, Hayashi M, Kiyohara E, Ando H, Terabe Y, Takami Y, Yamamoto K, Takeya Y, Takemoto M, Koshizaka M, Ebihara T, Nakamura A, Nishikawa M, Yao XJ, Hanaoka H, Katayama I, Yokote K, Rakugi H.(2018) Physician-initiated clinical study of limb ulcers treated with a functional peptide, SR-0379: from discovery to a randomized, double-blind, placebo-controlled trial. NPJ Aging Mech Dis. 2018 Feb 13;4:2.
Mori S, Zhou H, Yamaga M, Takemoto M, Yokote K(2017)Femoral osteoporosis is more common than lumbar osteoporosis in patients with Werner syndrome. Geriatr Gerontol Int. , 17(5):854-856.
Recent Trends in WRN Gene Mutation Patterns in Individuals with Werner Syndrome. Yamaga M, Takemoto M, Takada-Watanabe A, Koizumi N, Kitamoto T, Sakamoto K, Ishikawa T, Koshizaka M, Maezawa Y, Yokote K. J Am Geriatr Soc. 2017 Apr 10.
Werner syndrome: a model for sarcopenia due to accelerated aging:Masaya Yamaga, Minoru Takemoto, Mayumi Shoji, Kenichi Sakamoto, Masashi Yamamoto, Takahiro Ishikawa, Masaya Koshizaka, Yoshiro Maezawa, Kazuki Kobayashi, Koutaro Yokote、Aging 2017 Jul 19. doi: 10.18632/aging.101265.
Yokote K, Chanprasert S, Lee L, Eirich K, Takemoto M, Watanabe A, Koizumi N, Lessel D, Mori T, Hisama FM, Ladd PD, Angle B, Baris H, Cefle K, Palanduz S, Ozturk S, Chateau A, Deguchi K, Easwar TK, Federico A, Fox A, Grebe TA, Hay B, Nampoothiri S, Seiter K, Streeten E, Pina-Aguilar RE, Poke G, Poot M, Posmyk R, Martin GM, Kubisch C, Schindler D, Oshima J. (2017) WRN Mutation Update: Mutation Spectrum, Patient Registries, and Translational Prospects. Hum Mutat. 38(1):7-15.
Ide K, Baba Y, Takemoto M, Koide H, Ide S, Yamaga M, Kobayashi K, Yokote K. (2017) Case of Werner syndrome complicated by adrenal insufficiency due to hypothalamic dysfunction. Geriatr Gerontol Int, 17(2):346-347.
Mitamura Y, Azuma S, Matsumoto D, Takada-Watanabe A, Takemoto M, Yokote K, Motoshita J, Oda Y, Furue M, Takeuchi S. (2016) Case of sarcomatoid carcinoma occurring in a patient with Werner syndrome. J Dermatol. 43(11):1362-1364.
Mitamura Y, Azuma S, Matsumoto D, Takada-Watanabe A, Takemoto M, Yokote K, Motoshita J, Oda Y, Furue M, Takeuchi S. Case of sarcomatoid carcinoma occurring in a patient with Werner syndrome.J Dermatol. 2016 Apr 14.Epub ahead of print.
Ide S, Yamamoto M, Takemoto M, Fujimoto M, Ide K, Kobayashi K, Yokote K. Improved Glycemic Control and Vascular Function and Reduction of Abdominal Fat Accumulation with Liraglutide in a Case of Werner Syndrome with Diabetes Mellitus. J Am Geriatr Soc. 2016 Mar;64(3):687-8.
Takemoto M, Yamaga M, Furuichi Y, Yokote K.Astaxanthin Improves Nonalcoholic Fatty Liver Disease in Werner Syndrome with Diabetes Mellitus.J Am Geriatr Soc. 2015 Jun;63(6):1271-3.
Shimamoto A, Yokote K, Tahara H.Werner Syndrome-specific induced pluripotent stem cells: recovery of telomere function by reprogramming.Front Genet. 2015 Jan 29;6:10.
Shimamoto A, Kagawa H, Zensho K, Sera Y, Kazuki Y, Osaki M, Oshimura M, Ishigaki Y, Hamasaki K, Kodama Y, Yuasa S, Fukuda K, Hirashima K, Seimiya H, Koyama H, Shimizu T, Takemoto M, Yokote K, Goto M, Tahara H.Reprogramming suppresses premature senescence phenotypes of Werner syndrome cells and maintains chromosomal stability over long-term culture.PLoS One. 2014 Nov 12;9(11):e112900.
Toda N, Ihara K, Takemoto M, Yokote K, Hara T.Endocrine and metabolic abnormalities in a girl with childhood Werner syndrome: case report.J Am Geriatr Soc. 2014 Jul;62(7):1404-5.
Oshitari T, Kitahashi M, Mizuno S, Baba T, Kubota-Taniai M, Takemoto M, Yokote K, Yamamoto S, Roy S.Werner syndrome with refractory cystoid macular edema and immunohistochemical analysis of WRN proteins in human retinas.BMC Ophthalmol. 2014 Mar 12;14:31.
Watanabe K, Kobayashi K, Takemoto M, Ishibashi R, Yamaga M, Kawamura H, Fujimoto M, Ishikawa T, Onishi S, Okabe E, He P, Yokote K.Sitagliptin improves postprandial hyperglycemia by inhibiting glucagon secretion in Werner syndrome with diabetes.Diabetes Care. 2013 Aug;36(8):e119.
Takemoto M, Mori S, Kuzuya M, Yoshimoto S, Shimamoto A, Igarashi M, Tanaka Y, Miki T, Yokote K.Diagnostic criteria for Werner syndrome based on Japanese nationwide epidemiological survey.Geriatr Gerontol Int. 2013 Apr;13(2):475-81.
Kitamoto T, Takemoto M, Fujimoto M, Ishikawa T, Onishi S, Okabe E, Ishibashi R, Kobayashi K, Kawamura H, Yokote K.Sitagliptin successfully ameliorates glycemic control in Werner syndrome with diabetes.Diabetes Care. 2012 Dec;35(12):e83.
Onishi S, Takemoto M, Ishikawa T, Okabe E, Ishibashi R, He P, Kobayashi K, Fujimoto M, Kawamura H, Yokote K.Japanese diabetic patients with Werner syndrome exhibit high incidence of cancer.Acta Diabetol. 2012 Dec;49 Suppl 1:S259-60.

ウエルナー症候群患者家族の会ホームページ
http://8nkanja.8nkazoku.justhpbs.jp/
2016年12月11日 千葉県(きぼーる)
2015年7月25日 千葉県(千葉大学病院)
2014年11月16日 千葉県(千葉大学病院)
2013年10月13日 千葉県(千葉大学病院第2講堂)
2013年6月5日 大阪国際会議場
2012年2月19日 東京国際フォーラム
2011年5月7日 マリンピア喜入
2010年11月14日 千葉大学医学部附属病院 第3講堂
2010年6月19日 中野サンプラザ
2016年11月27日 関西地区会 大阪府吹田市(大阪大学最先端医療イノベーションセンター)
2015年11月29日 近畿中部地区会 愛知県名古屋市(日本ガイシフォーラム)
2015年11月25日 九州地区会 熊本県(荒尾市民病院)
2015年6月13日 中国地区会 広島県(福島生協病院)
2013年10月20日 近畿・中部地区集会~愛知県名古屋市(ウィルあいち)
2013年10月19日 九州地区集会~福岡県福岡市(ホテルセントラーゼ博多 ザ・ラウンジ)
2013年10月14日 中国地区集会~広島県広島市(広島大学)
2012年12月22日 近畿・中部地区集会~愛知県名古屋(ウィルあいち)
2012年10月16日 九州地区集会~福岡県(ホテルセントラーゼ博多 ザ・ラウンジ)
2012年7月8日 関東地区集会~千葉県(千葉大学病院第2講堂)
2011年12月11日 九州地区集会~佐賀県鳥栖市
2011年11月28日 近畿地区集会~奈良北葛城郡広陵町
Rothmund-Thomson Syndrome Foundation
ご相談、ご質問は werner.chiba(ここにアットマーク)gmail.com まで